
Mon - Sat 9:00 - 17:30
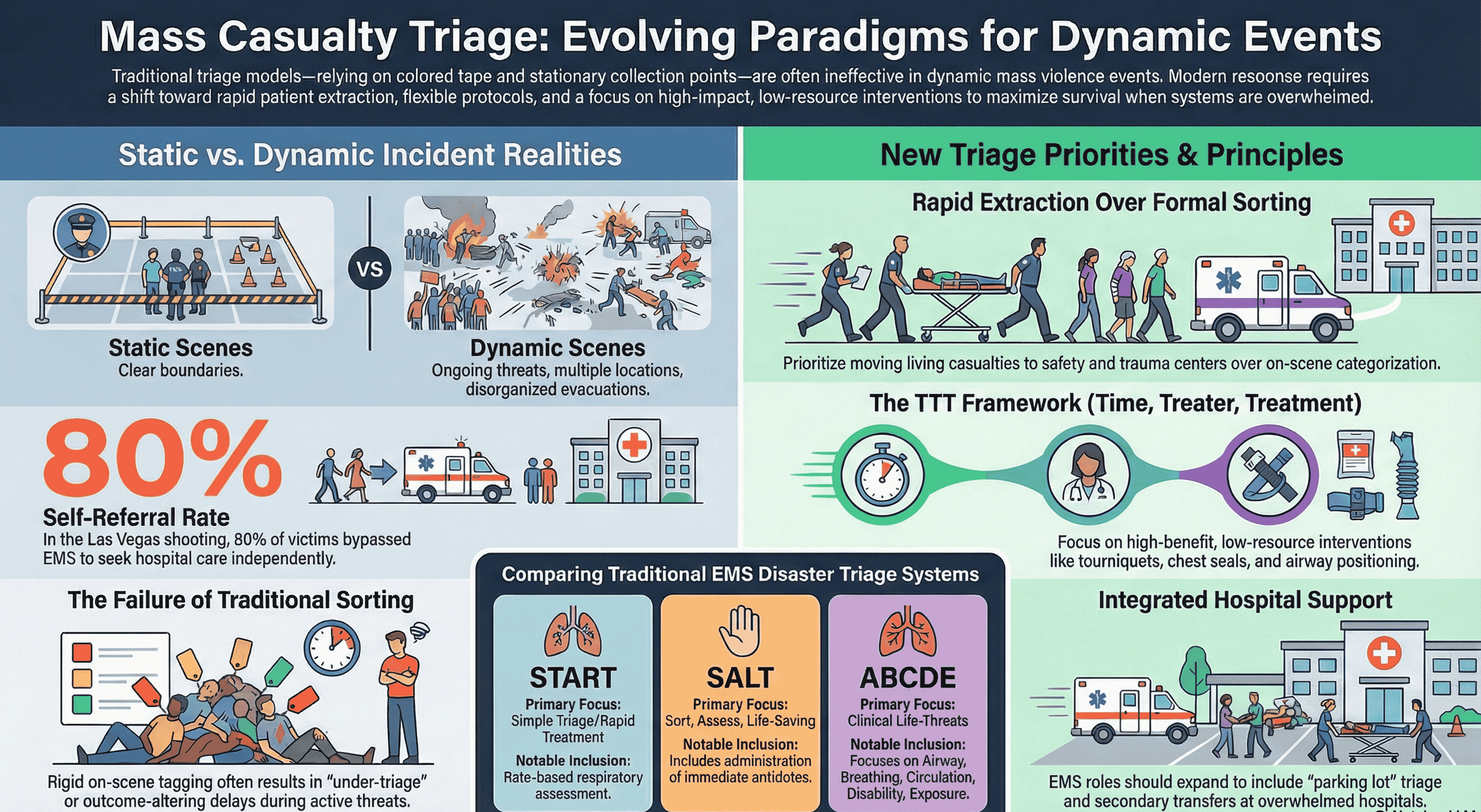
Mass casualty incident (MCI) management is undergoing a strategic evolution, moving away from "conventional" linear models that rely on static casualty collection points, backboards, and the meticulous application of colored tape. Modern incidents—characterized by mass violence and complex environmental threats—have exposed the lethal delays inherent in these rigid structures. We must transition to a dynamic framework where triage is understood not as a simple clinical assessment, but as a strategic assignment of resources. When medical systems are overwhelmed, the clinical objective shifts from individual definitive care to the tactical distribution of personnel, time, and equipment to mitigate systemic collapse.
Based on the ASPR TRACIE guidelines, the core goals of mass casualty triage are:
Strategic efficiency is dictated by the Time/Treater/Treatment (TTT) framework. This framework evaluates interventions based on three variables: Time (duration of the task vs. urgency), Treater (required level of expertise), and Treatment (volume of resources required). Under TTT, the most efficient interventions are those providing high benefit with minimal resource commitment, such as tourniquets or chest seals. Conversely, procedures requiring specialty staff and significant time are the least efficient in a surge. Identifying the specific nature of an incident is the prerequisite for applying this framework effectively.
Correctly characterizing an event is vital for responder safety and patient outcomes. The ASPR TRACIE guidelines define a Dynamic Incident as one where the scene is poorly defined, the threat is evolving, and the geography prevents the establishment of traditional medical structures. The Bhiwadi chemical factory fire serves as a quintessential dynamic incident, presenting a disorganized evacuation and shifting environmental hazards.
|
Incident Characteristic |
Specific Challenge to Traditional EMS Structures |
Antidote/LSI Timing & Impact |
|
Potential for Secondary Explosions |
Prevents fixed "Cold Zone" collection points; necessitates rapid, tiered extraction. |
Immediate need for hemorrhage control before moving; delay for sorting is lethal. |
|
Chemical Exposure |
Requires integrated decontamination to prevent system-wide contamination. |
SALT protocol allows antidote administration during assessment, reversing life threats immediately. |
|
Multiple Egress Points |
Impedes situational awareness; EMS cannot capture all patients at a single point. |
Victims may bypass LSIs entirely; requires mobile triage teams rather than fixed points. |
|
High Potential for Victims to Flee |
Leads to 80% self-referral rates, bypassing on-scene triage and overwhelming local EDs. |
"Sort then Treat" fails; patients arrive at hospitals with unaddressed internal chemical/thermal trauma. |
In a dynamic chemical fire, traditional structured triage often fails. As Dr. Edward Racht of American Medical Response observed, "I don’t think it does much to inspire confidence in EMS if we are seen focusing on opening and applying packages of triage tags when people need immediate care." In the Bhiwadi context, delays caused by "structuring" the scene result in avoidable mortality. Dynamic factors necessitate a flexible approach that prioritizes movement and rapid intervention over formal tagging.
Triage is a continuous process of re-evaluation, not a one-time event. For the victims of the Bhiwadi incident, the framework must be applied across three distinct levels:
Responders often face discomfort with the "Expectant" (Gray) category. However, clinicians must respect the TTT framework's resource-to-benefit ratio; in extreme surges, focusing on the moderately injured rather than the questionably salvageable may save more lives.
Managing chemical-related injuries requires recognizing unique physiological demands. Strategic planning must integrate LSIs—including hemorrhage control, airway positioning, and rapid antidote administration—directly into the triage flow.
Decontamination and Systemic Risk Decontamination is not merely a clinical task; it is an operational safeguard. Contaminated patients represent a catastrophic risk of secondary contamination to transport vehicles. A single contaminated patient can disable an entire ambulance or force the closure of an Emergency Department, effectively removing critical assets from the response system.
The ABCDE assessment framework must be adapted for these complexities:
Strategic readiness requires all congregate venues to have at least 20 "Stop the Bleed" kits co-located with AEDs to facilitate immediate bystander intervention.
Operational efficiency depends on synergy between EMS, Fire, and Law Enforcement via Unified Command.
The Rescue Task Force (RTF) Model In dynamic scenes, RTFs—combined teams of EMS and Law Enforcement—operate in "warm zones." Their objective is point-of-injury care and rapid extraction rather than waiting for a "cold zone" to be established.
The Role of Dispatch Dispatchers are the "first" first responders and must be empowered to deviate from scripts when the system is overwhelmed. Key roles include:
Hospitals must prepare for the reality that 80% of victims will arrive via self-referral, often bypassing on-scene triage.
EMS as a Force Multiplier As on-scene operations conclude, EMS assets must be redirected to support overwhelmed hospitals through "Parking Lot Triage." This allows hospitals to use EMS expertise for secondary transfers of less critical patients to non-trauma facilities, "off-loading" specialized centers.
Metric-Based Capacity Management The "polling" of hospitals for bed capacity is a fallacy—it is time-consuming and often inaccurate. Instead, hospitals must use specific metric-based triggers to signal saturation, such as:
Communication should be managed via Remote Clinical Command and in-person EMS/Hospital Liaisons. Furthermore, hospital primary triage should be performed by experienced providers—specifically those with military or field experience—who are accustomed to rapid, high-stakes categorization.
Resilience is built through "muscle memory" training that favors adaptive principles over rigid protocols. The goal is to move from equipment-heavy models to scalable, flexible systems.
Lessons Learned Checklist for Emergency Planners:
By adopting these principles, we move from rigid systems toward adaptive management, ensuring the greatest good for the greatest number in the most unpredictable environments.
We offer a full suite of HSEFS services designed to address your specific challenges and goals :
HSE Consulting & Advisory,
HSE Auditing & Assurance,
HSE Training & Development,
Implementation & Support,
Environmental Services
GST: 24ABDCA0826H1Z3
CIN: U71100GJ2025PTC163795
Copyright 2025. Agni Raksha Niti Engineering Consultancy Services Pvt. Ltd. All Rights Reserved.